All published articles of this journal are available on ScienceDirect.

The Perception of Physical Health Status in Obsessive-Compulsive Disorder: A Systematic Review and Meta-Analysis
Abstract
Background:
Physical Health Status is a neglected outcome in clinical practice with Obsessive-Compulsive Disorder (OCD) and a systematic review is lacking.
Objective:
The current study presents the first systematic review and meta-analysis summarizing the evidence on (a) perceived Physical Health Status, Bodily Pain and Role Limitations due to Physical Problems in patients with OCD compared with controls, (b) age, gender, severity of OCD symptoms, study publication date, study methodological quality as moderators of perceived Physical Health Status.
Methods:
Case-control studies were included if they (a) compared OCD patients with healthy/general population participants as controls, and (b) used validated self-report instruments. Two reviewers searched electronic databases, contacted corresponding authors, and examined reference lists/conference proceedings/theses.
Results:
Fourteen studies were included. A large significant negative effect size without publication bias showed that controls reported higher perceived Physical Health Status than patients with OCD. Medium and small effect sizes favouring controls emerged for Role Limitations due to Physical Problems and Bodily Pain, respectively. Higher age, females percentage, and publication date were associated with larger effect sizes; higher OCD severity and methodological quality were associated with smaller effect sizes.
Conclusion:
Perceived Physical Health should be evaluated and addressed by clinicians during treatment, particularly with older, female and less severe patients. Lifestyle interventions might be implemented.
1. INTRODUCTION
Obsessive-Compulsive Disorder (OCD) is a chronic mental health condition consisting of distressing thoughts, mental images or impulses, called obsessions, and recurrent overt/ mental behaviours, called compulsions [1]. Considerable evidence indicates that OCD produces a significant impairment in various health-related domains, such as interpersonal relation ships, intimate bonds, and work functioning [2-7]. Impairment in psychological quality of life is particularly severe for female patients and among those patients with less intense symptoms, as an inverse correlation between the intensity of OCD symptoms and quality of life there has been found [8].
While there is a long tradition of literature on the psychological quality of life in OCD, there is a paucity of evidence about perceived Physical Health Status, which is under-recognized by researchers and practitioners, as the focus of the intervention is often on the mental health dimension of the condition, such as obsessions and compulsions [9]. The rationale for investigating perceived physical health in OCD is related to various clinical aspects.
First, approximately 50% of patients suffer from concurrent general medical diseases [9]. Female and older patients with OCD are at a higher risk of developing general medical diseases [9]. Therefore, practitioners treating this clinical subgroup should be aware of this aspect and also evaluate and address this potential perceived impairment of physical health. Secondly, longitudinal research shows that OCD is associated with an increased physical health burden and double the risk of mortality compared with the general population [10] which remains elevated even after controlling for other concurrent mental health conditions [10]. Thirdly, specific OCD subtypes, such as contagion obsessions and doubts related to the possibility of causing harm, may have a physical health focus [11, 12]. For instance, contamination fears and engagement in repetitive washing behaviours can lead the patient to avoid social contacts or sports or to follow unhealthy eating habits. Moreover, there is an overlap in the cognitive and behavioural maintenance mechanisms of OCD and health anxiety, such as anxiety sensitivity and reassurance seeking [13, 14].
Fourthly, investigating physical health in OCD may suggest some clinical implications useful for practice. Physical health could be a target of treatment. The detrimental effects of OCD on perceived physical health might be due to the lack of a healthy lifestyle produced by the symptoms [9]. Some studies showed that interventions aimed at improving bodily health such as aerobic exercise in addition to standard treatment produce an improvement also in the OCD clinical picture and the related symptomatology, such as anxious symptoms and negative mood [15, 16]. OCD may be expected to benefit also from mindfulness-based interventions [17], which help the person decentering from intrusive thoughts and developing a not-judgemental attitude towards the body [18, 19].
Therefore, we may expect that OCD patients report poorer perceived physical health than controls without a psychiatric disorder or recruited from the general population. Certain sociodemographic variables, including age and gender, might act as moderators of a lower perceived physical health in OCD. The moderator role of age may be supported by previous research suggesting that the risk of general medical diseases among OCD patients is higher in older individuals than in younger ones [9]. Additionally, empirical evidence demonstrated gender-based clinical differences in OCD: female patients with OCD might experience worse physical health since they more frequently suffer from concurrent medical diseases, depressed mood, contamination fears, suicidality, and eating disorders, which potentially produce impairment in perceived physical health [20]. The severity of OCD symptoms might be expected to moderate the negative effect of the condition on physical health in the same manner as for psychological quality of life since lower severity is associated with impaired psychological quality of life [8].
In light of all these aspects, an insight into perceived physical health in OCD appears necessary and identifying which variables are associated with lower physical health in OCD can suggest some directions for clinical practice. In the present literature, there is no quantitative summary of perceived physical health in OCD patients. This study presents the first systematic review and meta-analysis aimed at summarizing the existing data on perceived physical health in OCD, specifically: (a) perceived Physical Health Status in OCD patients compared with controls (screened healthy individuals or individuals recruited from the general population), (b) socio-demographic, clinical, and study-related moderator variables of perceived Physical Health Status (age, gender, level of severity of OCD symptomatology, publication date, methodological quality), (c) additional outcomes related to perceived Physical Health Status, including Bodily Pain and Role Limitations due to Physical Problems.
2. METHODS
2.1. Eligibility Criteria
A systematic review was conducted following the PRISMA guidelines [21]. The protocol of the review was regisStered on PROSPERO (2018 CRD42018106194). Eligibility criteria involved (a) Characteristics of participants, (b) ChaSracteristics of outcomes, (c) Characteristics of comparators, (d) Characteristics of design:
(a) Studies were included if they used a clinical group with a current primary OCD diagnosis. Diagnosis had to be established by a semi-structured clinical interview based on the criteria of a standardized diagnostic system such as the Structured Clinical Interview according to DSM-IV [SCID-I; 22] or by an unstructured clinical interview conducted by a mental health professional based on the criteria of a standardized diagnostic system such as the DSM-5 [1] or the ICD-10 [23]. Studies including patients with a lifetime diagnosis of OCD or including participants with subthreshold OCD were not included. Studies were included only if they used adolescent/adult participants, as the clinical characteristics of the disorder in children are significantly different than those of adolescent/adult OCD [24]. Studies using participants with primary hoarding were excluded since it is conceptualized as a distinct diagnosis in the DSM-5. Studies were included if they had recruited patients from primary, secondary or tertiary care settings. Concurrent psychological or pharmacological treatment was not a reason for exclusion. Studies were not considered to be excluded if the patients had concurrent general medical diseases. Studies conducted on OCD in the elderly where patients included individuals aged over 70 years old, were excluded.
(b) Studies were included if they evaluated perceived Physical Health Status by validated, internationally recognized self-report instruments, such as the Medical Outcomes Survey 36-Item Short-Form Health Survey [36; 25] or the World Health Organization Quality of Life-Brief Form [WHOQOL-BREF; 26].
(c) Studies were included if using control groups of screened participants not meeting the criteria for any of the mental disorders included in a standardized classification system and this condition was checked by a clinical interview by a mental health practitioner. In addition, studies were also included if they used control groups of unscreened participants drawn from the general population.
(d) Studies were included if they used a case-control design, where a group of patients with a current primary OCD diagnosis was compared with a healthy or a general population control group on perceived physical health. Any other type of research was allowed if the study provided the data necessary to compute an effect size estimate (for the data requested to compute the effect sizes, see paragraph “Meta-analysis and summary measures”). No publication data or language restriction was applied.
2.2. Search Procedure
Studies were identified by carrying out an online systematic search of electronic databases and by using each of the keywords “Obsessive Compulsive Disorder”, “Obsessions”, “Compulsions” combined through the Boolean operator AND with the keywords “Physical Health”, “Physical Health Status”, “Physical Quality of Life”. The search procedure was conducted during the last week of November 2018 by using the electronic databases Scopus, PubMed, PsycINFO, EMBASE, Cochrane Library.
Subsequently, the corresponding authors of the included studies were contacted to request further data/to discover if they had further data. An inspection of all the references of the studies included in the review was also performed. An hand-search of conference proceedings was carried out in order to locate potential abstracts, papers, or posters relevant to OCD research presented at the following scientific associations: American Psychiatry Association, American Psychological Association, European Psychiatry Association, European Association of Psychology, British Psychological Society, Royal College of Psychiatrists. Theses and doctoral dissertations were hand-searched to identify additional unpublished eligible data.
2.3. Study Selection Process
Studies were assessed on eligibility criteria by two reviewers (AP, FF) independently during three different stages. During the first and the second stages, studies were assessed with regard to eligibility criteria after the reading of the title and of the abstract, respectively. During these stages, studies were retained when there was no agreement on inclusion between the reviewers. Finally, the studies remaining were assessed on eligibility criteria after the reading of the full text. In this selection stage, the reviewers discussed reasons for inclusion and any disagreements in judgement were addressed during meetings with another independent reviewer (AC) to obtain consensus on which studies to include in the pool.
2.4. Data Extraction and Coding
All the information was extracted from each of the included studies by two reviewers (AP, FF) independently and inserted into an excel worksheet which was firstly piloted on 2 included studies. The following information was extracted and coded from each of the studies: (a) Title of the paper, (b) First author, (c) Publication date, (d) Country where the study was conducted, (e) Inclusion and exclusion criteria, (f) Total sample size, (g) Number of patients with OCD, (h) Number of controls, (i) Types of controls (screened participants without psychiatric disorders or unscreened participants from general population), (j) Mean and standard deviation of the OCD group on the perceived Physical Health Status outcome, (k) Mean and standard deviation of the control group on the perceived Physical Health Status outcome, (l) Mean and standard deviation of the OCD group on the measure of role limitations due to physical problems, (m) Mean and standard deviation of the control group on the measure of role limitations due to physical problems, (n) Mean and standard deviation of the OCD group on the measure of bodily pain, (o) Mean and standard deviation of the control group on the measure of bodily pain, (p) Total mean age and age range, (q) Total percentage of females, (r) Measure(s) used to assess perceived Physical Health Status, (s) Measure(s) adopted to evaluate role limitations due to physical problems, (t) Measure(s) to assess bodily pain, (u) OCD symptom severity (measured in terms of the Y-BOCS scores), (v) Research design, (w) Instrument(s) used to establish the OCD diagnosis, (x) Percentage of patients on concurrent medication, (y) Patients’ recruitment strategies, (z) Strategies used to recruit the controls, (aa) Comorbid personality disorders, (ab) Comorbid depression symptoms, (ac) Percentage of patients with concurrent general medical diseases.
The third independent reviewer (AC) not involved in the extraction procedure checked the correctness of the data inserted in the worksheet by the other two reviewers. After the insertion of the data was completed, discrepancies in the data extracted by the two reviewers were discussed and resolved in a final meeting between the reviewers who conducted the data extraction and the third independent reviewer.
2.5. Moderator Coding
When inconsistency analyses showed significant and high heterogeneity between the effect sizes, the role of moderators was investigated. Two independent reviewers (FF and AP) coded the moderators independently. Subsequently, during meetings between the two reviewers, data insertion in the worksheet was checked for accuracy and potential discrepancies were resolved with a third reviewer (AC). The following variables were coded as moderators: (a) mean sample age; (b) sample gender (coded as the percentage of females); (c) OCD symptom severity, coded as a continuous variable based on Yale-Brown Obsessive Compulsive Scale scores [Y-BOCS; 27], which is the gold standard symptom measure; (d) study publication date; (e) study methodological quality according to the Newcastle-Ottawa Scale scores [NOS; 28] (see Quality Assessment paragraph below).
2.6. Quality Assessment
The NOS was used to judge the methodological quality of the studies. This tool has recently been recommended by systematic review practice guidelines as the most reliable instrument for conducting a quality assessment of cross-sectional/cohort studies [29]. The NOS includes eight items grouped into three domains: (a) Selection, (b) Comparability, (c) Outcome (cohort studies) or exposure (case-control studies) according to the study design. For each item, a series of response options are provided. A star system is adopted to allow a semi-quantitative quality assessment. The highest quality studies are assigned a maximum of one star for each item, excepting the item related to comparability where two stars are allowed. The scores on the NOS range from zero to nine stars. Two reviewers (AP, FF) performed the quality assessment independently. Discrepancies in the assignment of the scores were resolved in a consensus meeting with an independent third reviewer (AC).
2.7. Meta-Analysis and Summary Measures
The meta-analysis was calculated using random-effect models, which assume that the included studies are drawn from populations of studies that systematically differ from each other [30]. Effect sizes were calculated as standardized mean differences (SMD) by computing the following formula reported in Cohen [31]: (MOCD-MCONTROL)/SDPOOLED, where MOCD is the mean of the OCD groups on the perceived Physical Health Status instruments (or the measure of role limitations due to physical problems or the measure of bodily pain), MCONTROL indicates the mean of the controls on that measure and SDPOOLED is the pooled standard deviation. The effect sizes were estimated with a 95% confidence interval and interpreted according to the criteria described by Cohen [31]: values equal to 0.80 or higher were judged as large, values up to 0.50 as medium, and values up to 0.20 as small. When a study reported the data on more than one instrument to assess Physical Health Status, such as on both the SF-36 Physical Health Status scale and the WHOQOL-BREF Physical Health Status scale, a mean effect size was calculated by combining the effect sizes related to the scores on all the instruments. A standardized mean difference was calculated separately also for the data obtained from the SF-36 Role Limitations due to Physical Problems scale to summarize the evidence about the perceived negative interference of physical health-related problems. Finally, a standardized mean difference was calculated separately also for the data obtained from the SF-36 Bodily Pain scale to summarize the data related to perceived physical pain in OCD.
To verify publication bias, three different procedures were adopted including the Duval and Tweedie's trim and fill procedure [32], the visual inspection of the funnel plot and the Egger test.
Sensitivity analyses were performed by computing the effect sizes only in the studies (a) using the SF-36 Physical Health Status scale, (b) using adults, (c) using healthy screened controls, (d) using OCD patients without general medical disorders.
To assess between-studies heterogeneity, two indices were used, the I2 [33] and the Q statistic [34], respectively. The I2 is expressed as a percentage attributable to variability rather than chance [33]. A value close to zero indicates homogeneity, whereas values of 25%-50%, 50%-75%, and 75%-100% indicate low, moderate, and high heterogeneity, respectively. The Q statistic is computed by summing the squared deviations of each study’s effect estimate from the overall effect estimate while weighting the contribution of each study by its inverse variance [35]. In the hypothesis of homogeneity among the effect sizes, the Q statistic follows a chi-square distribution with k − 1 degrees of freedom, k being the number of studies. The moderators' analysis was conducted by performing weighted least squares meta-regressions. The meta-analysis was carried out using the Comprehensive Meta-analysis software version 2.00.
3. RESULTS
3.1. Study Selection
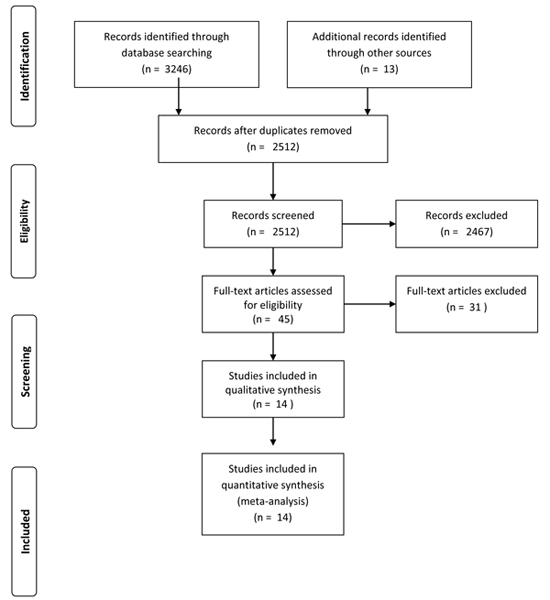
The electronic search and the search through additional sources produced 2512 records after removing duplicates. Of these, 2467 were excluded by the title or abstract as being on irrelevant constructs. Thus, 45 studies were full-text screened for inclusion. Sixteen studies were excluded for not using Physical Health Status measures or not assessing Physical Health Status/Role Limitations due to Physical Problems/Pain. Nine studies were excluded as they did not include a control group. Six studies were excluded since they were conducted on child samples. After this selection, fourteen studies were included by the consensus of the three independent assessors in the systematic review and meta-analysis (n= 20,223, 15 effect sizes). The Flow Chart is shown in Fig. (1).
3.2. Study Characteristics
All included studies were in English and published in peer-reviewed journals. Publication date ranged from 1996 to 2018. Three studies were conducted in Europe [36-38], three in North America [39-41], three in South America [5, 42, 43], three in Asia [44-46], two in the Middle East [47, 48]. All studies used adults, except for one [44] using adolescents/ adults (age range = 16 -70 years) and one using adolescents [42]. Six studies compared OCD patients with screened healthy controls [40, 42, 44, 46-48], eight compared OCD patients with controls recruited from the general population [5, 36-39, 41, 43, 45]. Eight studies used the SF-36 Physical Health Status scale [5, 36, 37, 39-41, 43, 48]; seven studies used the WHOQOL-BREF Physical Health Status scale [38, 39, 42, 44-47]. The included studies used different measures of depression: four studies [36, 37, 39, 48] used the HAM-D, three [5, 42, 44] used the BDI or the BDI-II, one [45] used the DASS-21, whereas the other studies did not assess depression.
Three studies [36, 38, 46] reported the proportion of the patients with personality disorders (51%, 0%, and 0%, respectively). Three studies [41, 44, 48] reported the proportion of the patients on concurrent pharmacotherapy (100%, 54%, and 100%, respectively). Five studies excluded patients with general medical disorders [5, 45-48], seven did not report information on comorbidity with general medical disorders [36, 38-40, 42-44], one reported that 74.60% of the group had comorbid medical disorders [37] and one reported 61.66% [41]. The supplementary file presents an overview of study characteristics.
3.3. Quality Assessment
Six studies received 5 points on the NOS [5, 38, 39, 41, 45], three received 6 points [36, 37, 47], four 7 points [40, 42, 44, 48] and one study [46] 9 points.
The definition of cases was judged as adequate for all the studies. All the studies were considered to have reported some independent validation. Representativeness of cases was judged as adequate for all the studies. Selection and definition of controls were judged as adequate for all the studies. Comparability of the subjects across the included studies was judged as adequate only in one study [46]. Ascertainment of exposure was judged as adequate for all the studies. Six studies did not use the same method of ascertainment of exposure for cases and controls and this item of the NOS was not judged as adequate for this subgroup of studies [5, 36-39, 41]. For six studies the provision of the information about the non-response rate was not judged as adequate [5, 38, 39, 47, 41, 45]. The quality assessment according to the criteria of the NOS is in Table 1.
3.4. Comparison of Perceived Physical Health Status between Patients with OCD and Controls
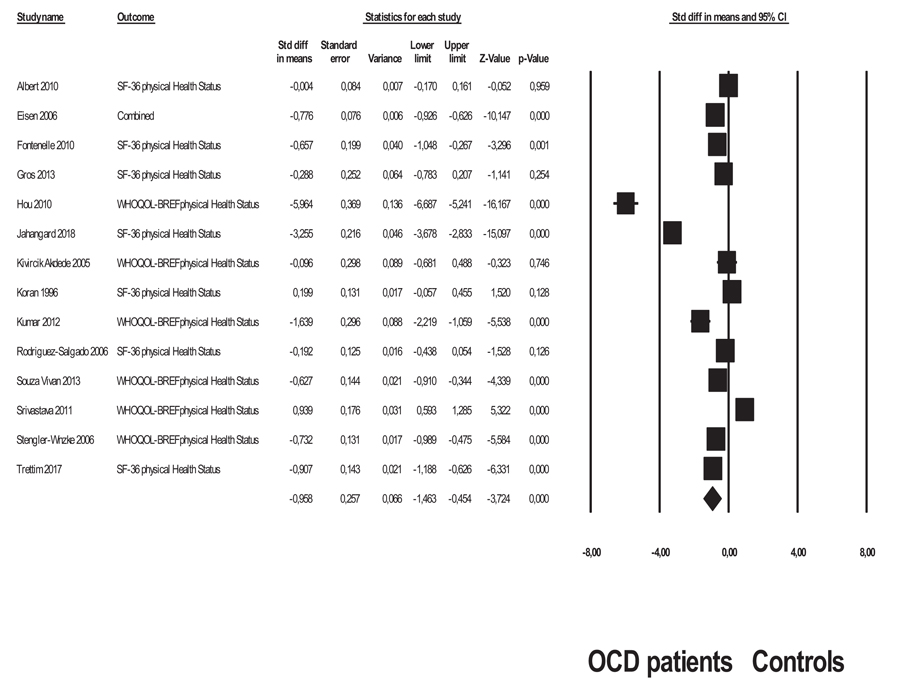
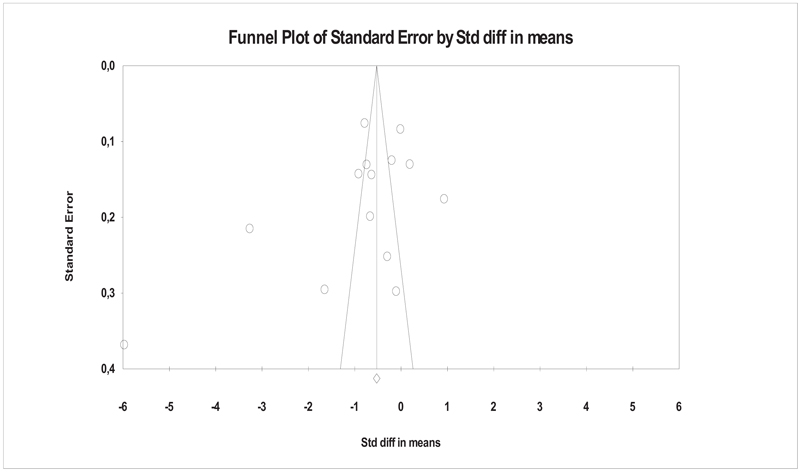
An overview of all the analyses is in Table 2. The comparison of perceived Physical Health Status showed a large significant-negative-effect size favouring controls over patients with OCD (SMD = -0.97, SE = 0.25, 95% CI: -1.46 - 0.45, p < 0.001). Controls reported significantly higher levels of perceived Physical Health Status than patients with OCD (Fig. 2). Evidence of publication bias was not observed as the values of the Egger test were not significant [B = -6.12, SE = 4.00, 95% CI: -14.86 - 2.60, t(12) = 1.52, p = 0.15] and the funnel plot did not appear asymmetrical (Fig. 3). Absence of publication bias was also supported by the trim and fill procedure showing that the mean effect size did not change when it was adjusted for publication bias (SMD = -0.95, 95% CI: -1.46 - 0.45; number of trimmed studies =0]. A significant heterogeneity was observed since the result of the Q test was significant [Q(13) = 560.80, p <0.001], and the value of the I2 was higher than 75 (I2 = 97.68).
| Study | Selection of Subjects | Comparability of Subjects | Exposure | Total Scores | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Definition of Cases | Representativeness of the Cases | Selection of Controls | Definition of Controls | Comparability of First Factor |
Ascertainment of Exposure |
Same Method of Ascertainment for Cases and Controls | Non-response Score | |||
| Albert 2010 | * | * | * | * | No | * | No | * | 6 | |
| Support for judgement and quote |
“A systematic face-to-face interview that consisted of structured and semistructured components was used to collect data from patients. Diagnostic evaluation and Axis I comorbidities were recorded by means of the Structured Clinical Interview for the DSM-IV Axis I Disorders. Personality disorders were ascertained with the Structured Clinical Interview for DSM-IV Axis II Disorders […] The interview and all the ratings were completed by psychiatrists with at least 4 year experience in anxiety and mood disorders”. “[…] We enrolled all consecutive patients with a principal diagnosis of OCD and with a YBOCS total score of 16 or greater who were referred to the Mood and Anxiety Disorders Unit of the University of Turin, Italy. This is a tertiary referral center located within the university hospital and specialized in the treatment of patients with OCD”. |
“The normative sample included 2031 Italian individuals drawn from the general population and who participated in the validation study of the Italian translation of the SF-36. The sample consisted of 999 (49.2%) males and 1031 (50.8%) females; their mean age was 47.73 (range, 18-96); 22.5% were single, 67.6% married, 8.0% widowed, and 2.0% separated”. | Cases and controls were not matched in the design and potential confounders were not adjusted for in the analysis. | “A systematic face-to-face interview that consisted of structured and semistructured components was used to collect data from patients. Diagnostic evaluation and Axis I comorbidities were recorded by means of the Structured Clinical Interview for the DSM-IV Axis I Disorders. Personality disorders were ascertained with the Structured Clinical Interview for DSM-IV Axis II Disorders […] The interview and all the ratings were completed by psychiatrists with at least 4 year experience in anxiety and mood disorders”. “We enrolled all consecutive patients with a principal diagnosis of OCD and with a YBOCS total score of 16 or greater who were referred to the Mood and Anxiety Disorders Unit of the University of Turin, Italy”. |
The study did not use the same method to ascertain exposure in cases and controls, since controls were unscreened participants | The study provided sufficient information about non-response rate “All patients gave their informed consent before enrolment in the study”. |
||||
| Eisen 2006 | * | * | * | * | No | * | No | No | 5 | |
| Support for judgement and quote | “Participants were 197 consecutive adult individuals recruited to be part of a 5-year prospective naturalistic study of course of illness in OCD. Inclusion criteria were 18 years or older, primary OCD (defined as the disorder participants considered their biggest problem overall), and treatment seeking. Recruitment was from a large OCD clinic, group psychiatric practices, psychologists’ offices, and mental health clinics in Rhode Island and Massachusetts”. “Interviewers went through a rigorous training process consisting of a training period, followed by a series of observed and taped interviews. Each case was presented at a weekly conference to review diagnoses and psychosocial impairment to ensure ongoing consistency in ratings”. |
“The community norms of the US general population (n = 2474) obtained from the validation study of the SF-36 (Ware, 1993)”. | Cases and controls were not matched in the design and potential confounders were not adjusted for in the analysis. | “Interviewers went through a rigorous training process consisting of a training period, followed by a series of observed and taped interviews. Each case was presented at a weekly conference to review diagnoses and psychosocial impairment to ensure ongoing consistency in ratings”. | The study did not use the same method to ascertain exposure in cases and controls, since controls were unscreened participants | The study does not provide sufficient information about non-response rate. | ||||
| Fontenelle 2010 | * | * | * | * | No | * | No | No | 5 | |
| Support for judgement and quote | “Volunteers for this study were consecutively recruited among patients undergoing treatment in the (1) Anxiety and Depression Research Program at the Institute of Psychiatry of the Universidade Federal do Rio de Janeiro (IPUB/UFRJ), the (2) Division of Applied Psychology at the Institute of Psychology of the same university (DPA/UFRJ) and (3) the first author’s private practice. The inclusion criteria were (1) the diagnosis of OCD, with or without psychiatric comorbidity confirmed by means of the Structured”. | “The control group consisted of community members recruited through local advertisements and included medical and administrative staff of the Universidade Federal do Rio de Janeiro. Inclusion criteria for the control group were (1) age between 18 and 80 years, and (2) the absence of any other neurological, endocrinological, or systemic disorder that could interfere with the interpretation of our results. Controls were not screened beforehand for the presence of psychiatric disorders, since we intended to avoid the selection of a ‘supernormal’ sample, which would be not representative of the general population”. | Although comparisons between cases and control were performed on demographic and clinical variables to test for the comparability of the two groups, cases and controls were not matched in the design and potential confounders were not adjusted for in the analysis. | “The diagnosis of OCD, with or without psychiatric comorbidity without psychiatric comorbidity confirmed by means of the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, fourth Edition, (DSM-IV) Axis I disorders”. | The study did not use the same method to ascertain exposure in cases and controls, since controls were unscreened participants | The study does not provide sufficient information about non-response rate. | ||||
| Gros 2013 | * | * | * | * | No | * | * | * | 7 | |
| Support for judgement and quote | “Veterans were randomly selected from a master list of patients who had attended a primary care appointment at one of four target VAMCs “Diagnostic criteria were based on the Diagnostic and Statistical Manual for Mental Disorders, Fourth Edition.2”. […]”Interviewers were master’s level clinicians trained and supervised by a licensed psychologist. Interview reliability was investigated through a random sample of interviews conducted via speakerphone by two interviewers (approximately 8%).” “Eligible patients were those who had been primary care attenders at any of the four target hospitals in fiscal year 1999. Stratifying on hospital, each patient was assigned a random number and the patient list ordered. According to this ordered list, blocks of 200 patients were sent to each hospital (new blocks were sent when these lists were exhausted)”. “Patients with known dementia, octogenarians and nonagenarians were excluded due to concern over ability to recall information critical to the study”. |
The control group consisted of veterans extracted from the sample reference population of cases | Although comparisons between cases and control were performed on demographic and clinical variables to test for the comparability of the two groups, cases and controls were not matched in the design and potential confounders were not adjusted for in the analysis. “Participants with OCD were significantly younger than participants without OCD (F=5.7; P=.02). No additional group differences were observed (χ2b1.8; PsN.17)”. | “Diagnostic criteria were based on the Diagnostic and Statistical Manual for Mental Disorders, Fourth Edition [13]. Interviewers were master’s level clinicians trained and supervised by a licensed psychologist. Interview reliability was investigated through a random sample of interviews conducted via speakerphone by two interviewers (approximately 8%)”. |
The study used the same method to ascertain exposure in cases and controls (DSM-IV criteria and MINI) | The study provided sufficient information about non-response rate “Afterwards, 854 participants (79.4%) completed follow-up phone interviews involving the Mini International Neuropsychiatric Interview (MINI) to assess current psychiatric disorders” |
||||
| Hou 2010 | * | * | * | * | No | * | * | * | 7 | |
| Support for judgement and quote | “From February to November 2008, 65 patients with OCD were consecutively recruited from the outpatient psychiatric clinics at a medical center and a regional teaching hospital in Southern Taiwan” “A psychiatrist systematically assessed all patients to confirm the diagnosis of OCD using the structured Mini-International Neuropsychiatric Interview [26] based on the diagnostic schemes of the 4th edition of the Diagnostic and Statistical Manual of Mental Disorders” |
“To recruit subjects for the control group, we posted an advertisement in the hospital and in newspapers to invite participation. A total of 157 persons responded to the advertisement. A psychiatrist assessed all responders systematically to determine whether they had any mood or psychotic disorders using the Mini-International Neuropsychiatric Interview. Those who had OCD, mood disorders, psychotic disorders, drank alcohol more than once per month, used any illicit drugs or had low mentality were excluded. A total of 106 subjects conformed to the criteria and were recruited as the control group“. |
Cases and controls were not matched in the design and potential confounders were not adjusted for in the analysis | “A psychiatrist systematically assessed all patients to confirm the diagnosis of OCD using the structured Mini-International Neuropsychiatric Interview [26] based on the diagnostic schemes of the 4th edition of the Diagnostic and Statistical Manual of Mental Disorders [27]”. |
The study used the same method to ascertain exposure in cases and controls (DSM-IV criteria and MINI) | The study provided sufficient information about non-response rate “From February to November 2008, 65 patients with OCD were consecutively recruited from the outpatient psychiatric clinics at a medical center and a regional teaching hospital in Southern Taiwan. Of these, five patients (3 men and 2 women) refused to participate in this study”. |
||||
| Jahangard 2018 | * | * | * | * | No | * | * | * | 7 | |
| Support for judgement and quote | “Outpatients diagnosed with OCD from the Farshchian Psychiatric Hospital in Hamadan (Iran) […] were approached to participate in the present cross-sectional and questionnaire-based study” “A total of 258 patients with OCD were approached and assessed against inclusion and exclusion criteria (see inclusion and exclusion criteria below). Inclusion criteria were as follows: (1) diagnosis by a psychiatrist of current OCD according to the DSM 5 (American Psychiatric Association, 2013); (2) Yale-Brown Obsessive Compulsive Scale (Y-BOCS; Goodman et al., 1989) score of 15 points or higher (see below); (3) no comorbid psychiatric disorders, except for diagnosis of a mild to moderate major depressive disorder, and no substance use disorder (SUD) of tobacco or cannabis or benzodiazepines; (4) no neurological, or other somatic disorders, as ascertained from patients’ reports and their medical records; (5) age between 18 and 65 years; (5) willing and able to participating in the study, and (6) written informed consent (see also Table 1). Exclusion criteria were: (1) acute psychosis and (2) acute suicidality (3) severe MDD and severe SUD of opioids, amphetamines/methamphetamines. The nature of the current treatment regimen (psychopharmacological treatment, psychotherapy, neuromodulation; combinations of such treatments) was not an exclusion criterion”. |
“[…] Healthy controls drawn from the hospital and university staff were approached to participate in the present cross-sectional and questionnaire-based study” “Healthy controls were recruited by advertisements on the homepage of the hospital and the University of Hamadan, and by word-of-mouth; during weekly staff meetings, staff members from different wards and departments of the university were encouraged to participate in the study and to ask and encourage other staff members to take part. Inclusion criteria were as follows: (1) age between 18 and 65 years; (2) no psychiatric disorders, as ascertained by a thorough neuropsychiatric” interview (Sheehan et al., 1998) conducted by trained psychiatrists and clinical psychologists; (3) no somatic illnesses, as ascertained by a thorough medical interview; (4) written informed consent”. |
Cases and controls were not matched in the design and potential confounders were not adjusted for in the analysis | “[…] diagnosis by a psychiatrist of current OCD according to the DSM 5 (American Psychiatric Association, 2013); (2) Yale-Brown Obsessive Compulsive Scale (Y-BOCS; Goodman et al., 1989) score of 15 points or higher (see below)”. |
The study used the same method to ascertain exposure in cases and controls (DSM-5 criteria and MINI) | The study provided sufficient information about non-response rate “As mentioned above (see inclusion and exclusion criteria in the Method section), a total of 258 patients with OCD were approached and after thorough assessment 117 (45,3%) were enrolled in the study. Of these, 17 patients (12.32%) declined participation; thus, the final sample consisted of 100 patients with OCD (72.46%)”. |
||||
| Kivircik Akdede 2005 | * | * | * | * | No | * | * | No | 6 | |
| Support for judgement and quote | “[…] subjects who were in follow up at out-patient clinic with the diagnosis of “Obsessive Compulsive Disorder” according to DSM-IV diagnostic criteria”. “Inclusion criteria were determined as absence of known physical or neurological disorder, Hamilton Depression Rating Scale less than 16 points and negative history of electro-convulsive therapy within last 6 months”. “All subjects were assessed by a psychiatrist initially. The patients who were diagnosed as obsessive-compulsive disorder and found to be eligible for the study in the first interview were directed towards a second investigator who was not unblinded to the diagnosis”. |
“Healthy individuals without self or family history of psychiatric diseases constituted the control group”. “All subjects were assessed by a psychiatrist initially. The patients who were diagnosed as obsessive-compulsive disorder and found to be eligible for the study in the first interview were directed towards a second investigator who was not unblinded to the diagnosis”. |
Although comparisons between cases and control were performed on demographic and clinical variables to test for the comparability of the two groups, cases and controls were not matched in the design and potential confounders were not adjusted for in the analysis. “There were no statistically significant differences between two groups in age, gender, hand preferences and educational level”. |
The study provides sufficient information about ascertainment of exposure. “[…] subjects who were in follow up at out-patient clinic with the diagnosis of “Obsessive Compulsive Disorder” according to DSM-IV diagnostic criteria”. “All subjects were assessed by a psychiatrist initially. The patients who were diagnosed as obsessive-compulsive disorder and found to be eligible for the study in the first interview were directed towards a second investigator who was not unblinded to the diagnosis”. |
The study used the same method to ascertain exposure in cases and controls (DSM-IV criteria). “All subjects were assessed by a psychiatrist initially. The patients who were diagnosed as obsessive-compulsive disorder and found to be eligible for the study in the first interview were directed towards a second investigator who was not unblinded to the diagnosis”. |
The study does not provide sufficient information about non-response rate. | ||||
| Koran 1996 | * | * | * | * | No | * | No | No | 5 | |
| Support for judgement and quote | ”At baseline an experienced clinical interviewer administered the Structured Clinical Interview for DSM-III-R (SCID) to establish psychiatric diagnoses” “We used the Yale-Brown Obsessive Compulsive Scale […] to quantify the severity of the patients’ obsessive compulsive symptoms”. |
“To compare the quality of life or our obsessive compulsive patients to the of the U.S. general population, we used U.S. population norms reflecting a representative sample of the non-institutionalized population.” | Cases and controls were not matched in the design and potential confounders were not adjusted for in the analysis. | ”At baseline an experienced clinical interviewer administered the Structured Clinical Interview for DSM-III-R (SCID) to establish psychiatric diagnoses” “We used the Yale-Brown Obsessive Compulsive Scale […] to quantify the severity of the patients’ obsessive compulsive symptoms”. |
The study did not use the same method to ascertain exposure in cases and controls, since controls were unscreened participants | The study does not provide sufficient information about non-response rate. | ||||
| Kumar 2012 | * | * | * | * | No | * | No | No | 5 | |
| Support for judgement and quote | “Consecutive patients (n=31) who satisfied study criteria were recruited between July 2008 and February 2009 from the Behavioral Medicine Unit of the NIMHANS” “Inclusion criteria for patients were age between 18 and 55 years, ability to read and write in English language, a primary diagnosis of OCD according to DSM-IV, and a score of 16 on the Y-BOCS. Patients who had severe comorbid psychiatric, physical and neurological disorders (i.e., psychosis, bipolar affective disorder, current psychoactive substance abuse or dependence, mental retardation, cancer, chronic pain, arthritis, asthma, head injury, and/or epilepsy), and those who had received exposure/response prevention or cognitive behaviour therapy (CBT)in the preceding year were excluded”. “The principal author performed all the evaluations using the following instruments: the mini International Neuropsychiatry Interview […]”. |
“Normal controls (n=30) comparable to patients with respect to age and gender were recruited by word of mouth from the local community. Only those who scored less than 2 on the General Health Questionnaire-12 were considered as normal controls”. | Although comparisons between cases and control were performed on demographic and clinical variables (e.g., depression and anxiety), and no difference emerged, except for education years, cases and controls were not matched in the design and potential confounders were not adjusted for in the analysis. | “[…] a primary diagnosis of OCD according to DSM-IV, and a score of 16 on the Y-BOCS […]” “The principal author performed all the evaluations using the following instruments: the mini International Neuropsychiatry Interview […]” |
The study did not use the same method to ascertain exposure in cases and controls, since controls were unscreened participants | The study does not provide sufficient information about non-response rate. | ||||
| Rodriguez-Salgado 2006 | * | * | * | * | No | * | No | * | 6 | |
| Support for judgement and quote | “Between November 2002 and November 2004, we recruited 64 adult patients (older than 18) with OCD diagnosis (according to DSM-IV criteria) at the psychiatric outpatient clinic at Ramon y Cajal General Hospital”. “All patients were interviewed by a clinical psychiatrist and assessed with the 5.0.0 Spanish version of the Mini International Psychiatric Interview (MINI) […]”. |
Spanish general population | Cases and controls were not matched in the design and potential confounders were not adjusted for in the analysis. | “All patients were interviewed by a clinical psychiatrist and assessed with the 5.0.0 Spanish version of the Mini International Psychiatric Interview (MINI) […]” | The study did not use the same method to ascertain exposure in cases and controls, since controls were unscreened participants | The study provided sufficient information about non-response rate “All of them agreed to participate in the study and signed a consent form”. |
||||
| Souza Vivan 2013 | * | * | * | * | No | * | * | * | 7 | |
| Support for judgement and quote | “All participants were recruited from a population-based, epidemiological study conducted with high school students from the city of Porto Alegre, southern Brazil, designed to assess the prevalence of OCD and obsessive-compulsive symptoms in adolescents”. “Subjects with OCD should meet the diagnostic criteria for the disorder according to DSM-IV 1 and score o 16 on the Yale-Brown Obsessive-Compulsive Scale (YBOCS)”. “Data were collected between May 2009 and August 2011. Adolescents were interviewed individually by previously trained psychologists at a university hospital (Hospital de Clınicas de Porto Alegre) or at their homes”. “The Brazilian version of the K-SADS-PL was used to confirm the diagnosis of OCD”. |
“Controls were randomly selected among participants; they had to score, 21 on the scale used to screen for obsessive-compulsive symptoms (Obsessive Compulsive Inventory - Revised, OCI-R) and should not have a diagnosis of OCD”. | Cases and controls were not matched in the design and potential confounders were not adjusted for in the analysis. “The two groups were significantly different in relation to sex (p = 0.008)”. |
“Subjects with OCD should meet the diagnostic criteria for the disorder according to DSM-IV 1 and score of 16 on the Yale-Brown Obsessive-Compulsive Scale (YBOCS)”. “Data were collected between May 2009 and August 2011. Adolescents were interviewed individually by previously trained psychologists at a university hospital (Hospital de Clınicas de Porto Alegre) or at their homes”. “The Brazilian version of the K-SADS-PL was used to confirm the diagnosis of OCD” |
The study used the same method to ascertain exposure in cases and controls (DSM-IV criteria and K-SADS) | The study provided sufficient information about non-response rate “Seventy six adolescents with OCD were identified, but one refused to participate in the present experiment”. |
||||
| Srivastava 2011 | * | * | * | * | ** | * | * | * | 9 | |
| Support for judgement and quote | “Forty five consecutive subjects with the diagnosis of OCD, according to the DSM-IV-TR criteria, from the psychiatry outpatients’ services of the University College of Medical Sciences and G. T. B. Hospital, a tertiary care hospital in Delhi were recruited for the study.” “The inclusion criteria of the OCD group were a) Subjects of either gender, aged ≥18 years with diagnosis according to the DSM-IV-TR criteria; b) Subjects included only newly diagnosed cases. The study excluded a) Subjects with past history or current evidence of schizophrenia, bipolar affective disorder, major depressive disorder, organic mental disorders and seizure disorders; b) Subjects having clinically significant and unstable renal, hepatic, cardio-vascular, respiratory or cerebrovascular disease or any other serious and progressive physical disease”. “Patients’ diagnoses of obsessive compulsive disorder and major depressive disorder were established by senior psychiatrist on the basis of history and clinical interview in accordance with DSM-IV criteria” “The diagnosis was reconfirmed by the principal author using the Mini-International Neuropsychiatry Interview (MINI)”. |
“A group of 150 healthy volunteers were included after excluding evidence of any psychiatric or medical/surgical illness after thorough history, physical examination and routine investigations (complete blood count, urinalysis, chest radiograph and electrocardiogram). The exclusion criteria were a) Subjects with past history or current evidence of schizophrenia, obsessive compulsive disorder, bipolar affective disorder, organic mental disorders and seizure disorders; b) Subjects having clinically significant and unstable renal, hepatic, cardiovascular, respiratory or cerebro-vascular disease or any other serious and progressive physical disease”. |
“The healthy control group was carefully matched with the OCD group with respect to potentially confounding variables like age and gender”. | “Patients’ diagnoses of obsessive compulsive disorder and major depressive disorder were established by senior psychiatrist on the basis of history and clinical interview in accordance with DSM-IV criteria” “The diagnosis was reconfirmed by the principal author using the Mini-International Neuropsychiatry Interview (MINI)”. |
The study used the same method to ascertain exposure in cases and controls (DSM-IV criteria and MINI) | The study provided sufficient information about non-response rate “Four patients declined participation in the study”. |
||||
| Stengler-Wenzke 2006 | * | * | * | * | No | * | No | No | 5 | |
| Support for judgement and quote | “Seventy-five patients (ICD-10 F42.0-F42.2; WHO 1993) treated in the outpatient clinic for patients with OCD and anxiety disorders at the Department of Psychiatry of the University of Leipzig were consecutively recruited”. | “In 2004 a representative survey was conducted in Germany among persons of German nationality who were aged 18 years and older and were not living in institutional settings. The sample was drawn using a random three-stage sampling: (1) electoral wards, (2) households, and (3) individuals within the target households. Target households within the sample points were determined according to the random route procedure; target persons were selected according to random digits. For our study only those respondents residing in Saxony, the state in which the city of Leipzig is located, were selected (n = 315)”. | Cases and controls were not matched in the design and potential confounders were not adjusted for in the analysis. | “[…] patients (ICD-10 F42.0-F42.2; WHO 1993)”. “Severity of OCD symptoms was assessed by the Yale-Brown Obsessive-Compulsive Scale […]”. |
The study did not use the same method to ascertain exposure in cases and controls, since controls were unscreened participants | The study does not provide information about non-response rate | ||||
| Trettim 2017 | * | * | * | * | No | * | * | * | 7 | |
| Support for judgement and quote | “The sample selection was performed by clusters, considering a population of 39.667 in the age range of interest according to the current census of 448 sectors in the city. To ensure the necessary sample size, 89 census-based sectors were randomly selected. Household selection in the sectors was performed according to a systematic sampling process, the first house being the one at the corner designated by IBGE (IBGE, 2008; http://ibge.gov.br) as starting the sector; every third house was selected”. “The study included seven interviewers, all of whom were undergraduate psychology or physical therapy students of Universidade Católica de Pelotas (UCPel). The interviewers were trained to administer the instrument by psychologists with extensive experience and weekly meetings were conducted throughout the data collection period. The interviews were conducted at home and lasted for about 40 minutes. After identifying the subjects, the interviewers were previously trained about the details of the application of instruments. The data were collected between August 2007 and December 2009. Young people that were unable to answer the diagnostic interview due to physical or cognitive problems were excluded”. |
Cases and controls were not matched in the design and potential confounders were not adjusted for in the analysis. | “Brazilian Portuguese validated version of the Mini Neuropsychiatric Interview (MINI) by Amorim (2000), a structured interview with proven validity and reliability, was used in the study”. |
The study used the same method to ascertain exposure in cases and controls, since controls were unscreened participants | The study does not provide information about non-response rate “Of the initial 1762 subjects identified for study inclusion, 11.5% refused to participate. Thus the final sample was composed of 1569 participants”. |
|||||
| Type of Analysis | k |
Effect Size (SMD) |
SE | p-value | 95% CI | Q(df) (p-value) | I2 | Evidence of Publication Bias |
|---|---|---|---|---|---|---|---|---|
| Random-effect Meta-analysis | ||||||||
| Comparison on Physical Health Status | 14 | -0.95 | 0.25 | <0.001 | -1.46-0.45 | 560.80(13) (<0.001) | 97.68 | No |
| Comparison on Bodily Pain | 6 | 0.22 | 0.05 | <0.001 | 0.11-0.33 | 6.50(59) (0.26) | 23.09 | No |
| Comparison on Role limitations due to physical problems | 6 | 0.55 | 0.14 | <0.001 | 0.83-0.26 | 41.59(5) (<0.001) | 87.98 | No |
| Sensitivity analyses | ||||||||
| Studies using SF-36 Physical Health Status scale | 8 | -0.63 | 0.26 | <0.05 | -1.15-0.10 | 244.49(7) (<0.001) | 97.13 | No |
| Studies using adult samples | 12 | -0.60 | 0.22 | <0.01 | -1.05-0.16 | 248.71(11) (<0.001) | 95.57 | No |
| Studies using screened controls | 6 | -1.53 | 0.83 | <0.001 | -3.16.0.09 | 432.99(5) (<0.001) | 98.84 | No |
| Studies excluding patients with comorbid medical conditions | 6 | -0.91 | 0.51 | 0.08 | -1.90-0.08 | 240.68(5) (<0.001) | 97.92 | Yes |
| Moderator analysis of Physical Health Status | k | B | SE | p-value | 95% CI | |||
| Age | 13 | -0.01 | 0.01 | <0.001 | -0.02-0.01 | |||
| Female gender | 14 | -0.03 | 0.01 | <0.001 | -0.04-0.02 | |||
| OCD severity (Y-BOCS scores) | 11 | 0.21 | 0.01 | <0.001 | 0.18-0.23 | |||
| Publication date | 14 | -0.05 | 0.01 | <0.001 | -0.06-0.03 | |||
| Methodological quality (NOS scores) | 14 | 0.10 | 0.03 | 0.008 | 0.02-0.16 |
3.5. Sensitivity Analysis
In a sensitivity analysis, the mean effect size was calculated by including only the studies (k = 8) using the SF-36 Physical Health Status scale [5, 36, 37, 39-41, 43, 48]. The results showed a medium significant effect size favouring controls over patients with OCD (SMD = -0.63, SE = 0.26, 95% CI: -1.15 - 0.10, p < 0.05). Evidence of publication bias was not observed as the result of the Egger test was not significant [B = -8.88, SE = 4.75, 95% CI: -20.851 - 2.74, t(6) = 1.86, p = 0.11]. Absence of publication bias was also supported by the trim and fill procedure which showed that the mean effect size did not change when it was corrected for publication bias (SMD = -0.63, 95% CI: -1.15 - 0.10; number of trimmed studies =0].
Another sensitivity analysis included only the studies using adults (k = 12) [5, 36-41, 43, 45-48]. A medium significant effect size emerged favouring controls over patients with OCD (SMD = -0.60, SE = 0.22, 95% CI: -1.05 - 0.16, p < 0.01). Evidence of publication bias was not observed as the Egger test was not significant [B = -2.52, SE = 4.06, 95% CI: -11.58 - 6.53, t(10) = 0.10, p = 0.54]. Absence of publication bias was also supported by the trim and fill procedure showing that the mean effect size did not change when corrected for publication bias (SMD = -0.60, 95% CI: -1.05 - 0.15; number of trimmed studies =0).
The mean effect size was calculated also by including only the studies using screened controls (k = 6) [40, 42, 44, 46-48]. The findings showed a large significant effect size favouring controls over patients with OCD (SMD = -1.53, SE = 0.83, 95% CI: -3.16 - 0.09, p < 0.001). Evidence of publication bias was not found as the Egger test was not significant [B = -14.65, SE = 12.23, 95% CI: -48.62 - 19.31, t(4) = 1.19, p = 0.29]. Absence of publication bias was supported by the trim and fill procedure which showed that the mean effect size did not change when it was corrected for publication bias (SMD = -1.53, 95% CI: -3.16 - 0.09; number of trimmed studies = 0).
A further sensitivity analysis included only the studies using patients without comorbid medical conditions (k = 6) [5, 39, 45-48]. The results showed a large yet non-significant effect size favouring controls over patients with OCD (SMD = -0.91, SE = 0.51, 95% CI: -1.90 - 0.08, p = 0.08). Evidence of publication bias was not found by the Egger test, which was non-significant [B = -1.45, SE = 6.35, 95% CI: -48.62 - 19.31, t(4) = 0.22, p = 0.82] but it was supported by the trim and fill procedure showing that the mean effect size changed when corrected for publication bias (SMD = -1.57, SE = 0.51, 95% CI: -1.90 - 0.08; number of trimmed studies = 2).
3.6. Comparison on SF-36 Bodily Pain between Patients with OCD and Controls
The comparison on bodily pain showed a significant, yet small, positive effect size favouring patients with OCD over controls (SMD = 0.22, SE = 0.05, 95% CI: 0.11 - 0.33, p < 0.001, k = 6): patients reported significantly higher levels of bodily pain than controls. No evidence of heterogeneity emerged [Q(5) = 6.50, p = 0.26, I2 = 23.09]. Absence of publication bias was supported by the trim and fill procedure showing that the mean effect size did not change when corrected for publication bias (SMD = -0.22, 95% CI: 0.11 - 0.33; number of trimmed studies =0) and confirmed also by the Egger test, which was not significant [B = 2.01, SE = 0.97, 95% CI: -0.70 - 4.73, t(4) = 2.06, p = 0.10].
3.7. Comparison on SF-36 Role Limitations due to Physical Problems between OCD Patients and Controls
The comparison of SF-36 Role Limitations due to Physical Problems showed a medium significant positive effect size favouring patients with OCD over controls (SMD = 0.55, SE = 0.14, 95% CI: 0.83 - 0.26, p < 0.001, k = 6): patients reported significantly higher levels of role limitations due to physical problems than controls. Significant heterogeneity emerged [Q(5) = 41.59, p < 0.001, I2= 87.98]. Absence of publication bias was supported by the trim and fill procedure showing that the mean effect size did not change when corrected for publication bias (SMD = 0.55, 95% CI: 0.83 - 0.26; number of trimmed studies =0). Absence of publication bias was confirmed also by the Egger test which was not significant [B = -1.60, SE = 3.45, 95% CI: -11.19 - 7.98, t(4) = 0.46, p = 0.65].
3.8. Moderator Analysis
Age was negatively associated with the effect sizes: higher age was associated with larger standardized mean differences in effect sizes on perceived Physical Health Status between patients with OCD and controls (B = -0.01, SE = 0.01, 95% CI: -0.02 - 0.01, p < 0.001, k = 13). Female gender was negatively associated with the effect sizes: higher percentage of females was associated with larger standardized mean differences in effect sizes on perceived Physical Health Status between patients with OCD and controls (B = -0.03, SE = 0.01, 95% CI: -0.04 - 0.02, p < 0.001, k = 14). OCD severity was positively associated with the effect sizes: higher OCD severity was associated with narrower standardized mean differences in effect sizes on perceived Physical Health Status between patients with OCD and controls (B = 0.21, SE = 0.01, 95% CI: 0.18 - 0.23, p < 0.001, k = 11).
Publication date was negatively associated with the effect sizes: more recent publication dates were associated with larger standardized mean differences in effect sizes on perceived Physical Health Status between patients with OCD and controls (B = -0.05, SE = 0.01, 95% CI: -0.06 - 0.03, p < 0.001, k = 14).
Methodological quality, coded through the scores on the NOS, was positively associated with effect sizes. Studies with higher methodological quality were associated with lower standardized mean differences in effect sizes on perceived Physical Health Status between patients with OCD and controls (B = 0.10, SE = 0.03, 95% CI: 0.02-0.16, p = 0.008, k = 14).
4. DISCUSSION
While there are numerous literature studies on the psychological quality of life in OCD [2, 3], perceived physical health is under-recognized as research and practice focus on the mental health component of the condition [9]. This investigation is the first systematic review and meta-analysis studying perceived Physical Health Status in patients with OCD. Fourteen studies were included. According to a range of NOS methodological quality points from 0 to 9, six studies received 5 points, three received 6 points, four studies 7 points and one study nine points. Perceived Physical Health Status was significantly lower in patients with OCD than in controls, as indicated by a large effect size without evidence of publication bias. This result was similar to the large effect size (SMD = - 1.22, p < 0.001) reported in a recent meta-analysis on patients with schizophrenia [49] where the clinical groups reported significantly lower perceived Physical Health Status than the control groups, as measured by the WHOQOL-BREF [26]. Although this has the limitation of indirect comparison, this result suggests that perceived physical health in OCD may be impaired to the same extent as in other severe psychiatric conditions such as psychoses.
In the studies using the SF-36 Physical Health Status scale, the effect size was medium without publication bias. A medium effect size without publication bias was also found when the analysis was conducted only on adults. A non-significant effect size emerged in those studies reporting that patients had not comorbid medical disorders, but this analysis included only 6 studies and appeared at risk of publication bias. Patients with OCD reported significantly higher Bodily Pain than controls without publication bias and heterogeneity. However, it should be noted that for Bodily Pain the effect size was small. Patients with OCD reported significantly higher levels of Role limitations due to physical problems than controls, with a medium effect size without publication bias. Overall, the present results suggest that in OCD, perceived Physical Health Status and Role Limitations due to Physical Problems are lower than among controls and should be considered as an important problem associated with this disease. The smaller difference between patients and controls on Bodily Pain suggests that this physical outcome may be less relevant to OCD. It might be hypothesized that OCD is associated with worse Physical Health Status due to an unhealthy lifestyle, including sedentary lifestyle, social isolation, unhealthy eating habits caused by contamination fears [11] or the use of maladaptive behaviours to regulate negative emotion, such as cigarette smoking. This point may have the implication of suggesting that clinicians also address physical health literacy during their psychiatric encounters with OCD patients. As these variables were not controlled for, future research should assess whether Physical Health status is worsened by an unhealthy lifestyle. Alternatively, it may be that patients with OCD have health anxiety and selective attention mechanisms on bodily signs leading to misinterpretations of them, and then to a worse perception of Health Status [14]. A clinical implication of this may be the use of interventions targeting anxiety sensitivity in OCD, which can reduce OCD symptoms by decreasing hypervigilance on body signs and misinterpretations of them [50]. Perceived Physical Health Status should be a target of treatment; the implication of these results may be that health-focused interventions may be included as adjuncts to standard treatment [15, 51, 52]. Also, mindfulness-based therapy may be useful for Physical Health in OCD as it enables the person to decenter from intrusive thoughts and have a non-judgemental attitude towards the body [17].
Higher age was associated with larger effect sizes on perceived Physical Health Status between patients with OCD and controls. This result may be attributed to the fact that perceived Physical Health tends to decrease over time and it may be lower for older patients. In addition, the effect of age may be a consequence of longer illness duration: symptoms persisting over time can reduce perceived Physical Health due to the cumulative effect of the above-mentioned variables associated with OCD interfering with Physical Health, such as social isolation and a sedentary lifestyle.
Female gender was negatively associated with effect sizes. A higher females percentage was associated with larger effect sizes on perceived Physical Health Status between OCD patients and controls. This result suggested that females had worse perceived Physical Health than males, consistent with the evidence found on psychological quality of life [3]. This result may be in line with a general trend in the scientific literature related to the so-called “Gender and health paradox” [53], indicating that women report worse health than men (despite living longer). Gender-based differences in the clinical picture of OCD may also explain the result that females tend to experience a worse physical health status. Females with OCD more frequently report medical diseases, negative mood, contamination fears, suicidal ideation, and comorbid eating disorders, which appear to impact the perception of physical health [20].
OCD severity was positively associated with effect sizes: higher OCD severity was associated with smaller differences in effect sizes on perceived Physical Health Status between OCD patients and controls. This result seemed to be consistent with the evidence found for psychological quality of life in OCD, which tends to be lower for patients with less severe symptoms than for those with higher severity [8]. An explanation may be that patients with less severe symptoms have higher health expectancies, that would make them have a worse perception of Physical Health Status. The clinical implication of this may be that clinicians should pay attention to perceived Physical Health of less severe patients. Publication date was negatively associated with the effect sizes: more recent publication dates were associated with larger differences in effect sizes on perceived Physical Health Status between patients with OCD and controls.
4.1. Limitations and Conclusion
Some shortcomings should be pointed out. Firstly, the cross-sectional design of the studies does not allow conclusions to be drawn about the causal effect of OCD symptoms on perceived physical health but can only suggest an association. It might be argued that a poorer perception of Physical Health Status can induce obsessive fears or exacerbate to some extent pre-existing fears or compulsive behaviours. Thus, the investigation of perceived physical health needs for prospective designs. Secondly, seven of the studies did not report information about comorbid medical conditions. This lack of information prevented the adjustment of the analyses, and the sensitivity analysis was conducted on a small subgroup.
Only three out of the studies provided information about the number of patients on concurrent psychopharmacological treatment: 100% of the samples in two studies [41, 44] and 54% in one [48]. The lack of this information does not allow the effects of psychopharmacotherapy on perceived physical health to be accounted for. It may be argued that medication routinely prescribed for OCD at higher dosages than for anxiety or depressive disorders, such as Selective Serotonin Reuptake Inhibitors (SSRIs), may be associated with side-effects that impact physical health such as nausea, dizziness sedation, insomnia, and sexual dysfunction [54]. In addition, since OCD is typically a resistant disorder, it is often necessary to associate different classes of drugs in addition to the SSRIs such as Atypical Antipsychotics, as evidenced also by a recent review [55], with the risk of greater side effects and less perception of one's health. Another variable potentially moderating the association between OCD and physical health might be depression [56, 57]. However, in the present studies there was a large heterogeneity in the instruments used to measure it and this did not allow depression to be investigated as a moderator. As previously mentioned, future research should compare perceived physical health in OCD with other severe mental disorders such as psychosis or potentially with other conditions belonging to the so-called OCD spectrum, such as body dysmorphic disorder or skin picking disorder which typically involve a negative body experience [58, 59].
In conclusion, this is the first systematic review on Perceived Physical health in OCD: this quality of life domain should be considered more carefully by researchers in future investigations and by clinicians as a target of treatment, particularly with older, female and less severe patients. New interventions for Physical Health status in OCD may be evaluated.
CONSENT FOR PUBLICATION
Written of informed consents were obtained from all the participants prior of the study.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
AP designed the study, wrote the protocol, searched the literature, participated in the selection of the studies, performed the statistical analysis, and wrote the paper.
FF designed the study, wrote the protocol, searched the literature, participated in the selection of the studies, performed the statistical analysis, and wrote the paper.
AC designed the study, participated in the selection of the studies, and reviewed and approved the final version of the paper.
SUPPLEMENTARY MATERIAL
Supplementary material is available on the publishers Website along with the published article.

