All published articles of this journal are available on ScienceDirect.

Antidepressant Prescribing and Suicides in Emilia-Romagna Region (Italy) from 1999 to 2008: An Ecological Study
Abstract
Anti-depressant (AD) prescribing rose in several countries worldwide over the last 20 years. Some concerns have been raised over the fact that AD use, mainly Selective Serotonin Reuptake Inhibitors (SSRI) may increase the risk of suicide. AD consumption and suicide rates data in Emilia-Romagna region, Italy have been extracted from regional government databases on AD prescribing and suicide rates, from 1999 to 2008. A statistical model using ordinary least squares linear regression was employed. The overall suicide rates decreased during the period under examination, in spite of the observed exponential increase in use of ADs. Despite the doubling in prescribing of SSRI and newer ADs in recent years, there continues to be no negative impact on suicide rates in Emilia Romagna.
INTRODUCTION
Anti-depressant (AD) prescribing rose in several countries worldwide over the last 20 years [1], mainly after the introduction of Selective Serotonin Reuptake Inhibitors [1, 2]. This increase may be the result of better treatment and recognition of depression [1]. There is some evidence that treating more depressed patients with AD might prevent suicide [3]. However, some concerns have been raised over the fact that AD use, mainly Selective Serotonin Reuptake Inhibitors (SSRI) may increase the risk of suicide [4]. Ecological studies showed some evidence that more widespread AD use corresponds to a decrease in suicide rates [1], although this finding is disputed [5]. A meta-analysis published in 2009 [6] showed that the risk in suicidality associated with use of antidepressants strongly depends on age, with a higher risk in adults aged 25 years of age or under, a reduced risk of suicidality among people aged 65 and older, and a possibly protective effect in adults aged 25 to 64 years.
The aim of this study is to investigate the trend in AD prescribing and deaths by suicide in Emilia Romagna, a large Italian region, with a view to understanding how the pattern of AD sale is related to suicide.
MATERIALS AND METHODOLOGY
Emilia-Romagna is a northern Italian region with a population of about 4.4 million people [7]. It has an area of 22446 km2.
Data concerning suicide rates based on ICD-IX classification (E950-E959) [8], were collected by the SALUTER database [9]. This is the official internet site for the Regional Government-funded statistical office on health- related statistics for Emilia-Romagna region. The rates were age-standardized per 100000 population by the statistical office, with the direct method, based on the 1998 resident population. Rates for males and females were extracted. Data are available from 1999 to 2008. No data have been released after 2008.
AD prescribing data were collected from the official government-funded CREVIF database [10]. This office collects data on all medication prescribed by the Italian National Health Service in Emilia-Romagna region. Every year the CREVIF issues a report outlining the Defined Daily Doses (DDD)/1000 population/day (DDDM) for each category or subcategory of medication, which is available on-line [10]. Data were not divided by age or sex. The DDD is the international unit of drug utilisation approved by the World Health Organisation for drug use studies [11]. The DDD is a theoretical unit of measurement defined as the assumed average maintenance daily dose for a drug, used for its main indication in adults. The DDDM indicates how many people per 1,000 of the population have in theory received a standard dose (i.e. the DDD) of a particular medication or category of medication daily. The ADs were aggregated by CREVIF into three categories: SSRI (fluoxetine, fluvoxamine, citalopram, escitalopram, sertraline, paroxetine), Tryciclic ADs (TCA), and Others (Mianserin, Trazodone, Mirtazapine, Venlafaxine, Reboxetine, Duloxetine). Data were available from 1999 to 2008. There is no data after 2008.
A statistical model using ordinary least squares linear regression was employed, based on the model developed by Preti and Miotto [12]. The model was used in the present study to test for changes over time in suicide rates. Rates were the dependent variable and years were the independent variable. Linear regression analysis of rates over 10 years (1999-2008) was performed. A two-tailed t-test was also performed to test for the hypothesis of a significant slope.
SPSS for Windows version 19 has been used to perform all the calculations.
RESULTS
Results on AD prescribing and suicides are shown on Fig. (1).
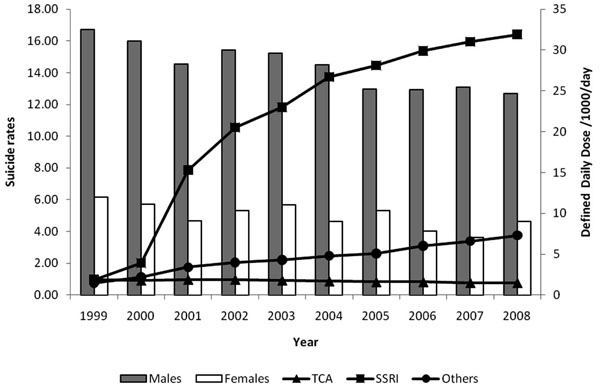
Suicide rates per 100.000 inhabitants (bars) and antidepressant drug consumption (lines) in Emilia-Romagna 1999-2008
The analysis of AD drug prescribing revealed that there has been a marked increase in the use of SSRI. The DDDM for SSRI increased from 1.9 in 1999 to 31.9 in 2008, more than 15-fold increase. DDDM for TCA, on the other hand, slightly decreased from 1.9 in 1999 to 1.5 in 2008. A nearly 5-fold increase in the prescription of other ADs has also been observed between 1999 and 2008, with a DDDM increasing from 1.5 in 1999 to 7.3 in 2008. Standardized suicide rates decreased in males from 16.70 in 1999 to 12.69 in 2008. In females, standardized suicide rates decreased from 6.15 in 1999 to 4.61 in 2008. The Linear Regression Model showed that there has been a slow but progressive decrease in suicide rates for males (slope= -0.440, 95% Confidence Interval= -0.581 to -0.299, Standard Error= 0.061, Adj R2= 0.850,F=51.99, p= 0.0001) and for females (slope= -0.199, 95% Confidence Interval= -0.340 to -0.057, Standard Error= 0.061, Adj R2= 0.567,F=10.50, p= 0.012).
DISCUSSION
The main finding of this study is that the overall suicide rates decreased during the period under examination, in spite of the observed exponential increase in use of ADs.
Our analysis showed that despite the doubling in prescribing of SSRI and newer ADs in recent years, there continues to be no negative impact on suicide rates in Emilia Romagna. If this findings were consistent to Healy’s and colleagues’ [4], prediction of an increase in suicide by SSRI, there would have been a marked increase in suicide rates, which did not happen. Also, Khan and colleagues showed that SSRI do not induce suicide more than other AD or even placebo [13]. Our findings are more in line with the data examined by Isaacson and colleagues for Europe and worldwide [1], where suicide rates showed an opposite trend to AD prescribing. If we consider the trend of suicides in Italy we notice that there has been a decrease in rates even before the appearance of SSRI in the Italian market. Guaiana and colleagues [14] found that there was an overall decline in suicide rates in Italy from 1986 to 1996, both in males and in females. However, suicides rates markedly declined among elderly of both sexes and increased in males aged 15-24 and 25-44. When suicide rates were compared to antidepressant prescribing in Italy, it appeared that there has been an overall steady decline in suicide rates, between 1955 and 2000, which preceded the exponential increase in AD prescribing [2]. This decrease may be linked to earlier treatment and detection of mental disorders. Vichi and colleagues also examined suicide rates in Italy between 1980 and 2002 [15]. They concluded that the decline in suicide rates is possibly a consequence of the decrease in the incidence of mental disorders as a result of the development of an integrated and community-based mental health system, which in turn may have led to decreased suicide rates. AD prescribing may be part of this picture, as earlier detection of mental disorder may have to an increase in AD prescribing. Mental illness in general and depression in particular are a strong predictor of suicide [16]. Earlier detection of depression by community mental health services might have led to increased treatment with AD that, in turn, led to a decrease in suicide rates. This hypothesis, however suggestive, remains speculative.
This study suffers from some obvious limitations: first of all, the naturalistic design makes it prone to the ecological fallacy, as no clear casual relationship can be established. Also, data on DDDM and suicides were not divided by age or sex. It is possible that the negative trend in suicide rates can be only applied to certain age groups, including the elderly. It appears that people over 65 account for the majority of AD prescribing in Italy [17] and suicides in Italy seem to decline mostly in people aged 65 or more [2]. It can be possible that the decrease in suicide rates observed in Emilia-Romagna applies mainly to people aged 65 or older, although we do not have data to confirm or refute this hypothesis. Also, we assumed that all ADs are prescribed and used for depression. This is not entirely true, as ADs are increasingly used for anxiety disorders as well, also in Italy [18]. Anxiety disorders are at least as prevalent as depression. Both types of disorders are highly comorbid. Our database does not make it possible to find out the specific disease that required the prescription of the AD. However, since anxiety and depression are closely intermingled, the former being often an indicator of the severity of the latter and vice versa [19], this limitation does not invalidate our main conclusions. Finally, data on AD sale does not capture actual AD consumption. It is definitely possible that people who are prescribed AD do not take them regularly or at all.
CONCLUSIONS
In spite of the limitations, we can say that an increase an AD prescribing (particularly SSRI) has not been paralleled by an increase in suicide rates in Emilia-Romagna region of Italy. Further studies will be required to refute or corroborate this finding.

